Hydroxychloroquin - Chloroquin
Dies ist eine veraltete Version, die durch die neuere englische Version ersetzt wurde.

Pharmacokinetische Daten
Quelle: Goodman & Gilman's "The Pharmacological Basis of Therapeutics", 9th edition (1996)
CHLOROQUINa
Verfügbarkeit (oral) (%): 89 ± 16
Ausscheidung mit dem Urin (%): 61 ± 4
In Plasma gebunden (%): 61 ± 9; ´ rheumatoid Arthritis
Clearance (CL/F, ml * min-1 * kg-1): 1.8 ± 0.4b
Verteilungsvolumen. (Vss/F, Liter/kg): 115 ± 61b
Eliminationshalbwertszeit (t1/2, Stunden): 41 ± 14
Tage,c
wirksame Konzentration: 15 ng/mld;
30 ng/mle
Toxische Konzentration: 0.25 mg/mlf
Schlüssel für Abkürzungen
a Aktiver Metabolit, Desethylchloroquin, trägt 20 ± 3%
der Ausscheidung mit dem Urin bei; t1/2 = 15 ± 6 Tage.
b Blut CL/F, Vss/F, und t1/2; Blut-zu-Plasma Konzentrationsverhältnis
= 9.
c Kürzere Halbwertszeiten wurden früher berichtet, wenn die
Probennahme nach einem Monat endete.
d Plasmodium vivax.
e Plasmodium falciparum.
f Doppeltsehen; Benommenheit.
Quelle:
White, N.J. Clinical pharmacokinetics of antimalarial drugs. Clin.
Pharmacokinet., 1985, 10:187-215.
(hinzugefügt durch J.
Gruber)
-
F = Körpergewicht,
-
Vss = Verteilungsvolumen im Gleichgewicht,
-
t1/2 = Eliminationshalbwertszeit,
-
CL/F Einheiten = ml Blut-Kompartment / (min kg Körpergewicht)
-
Setzt man das Körpergewicht (z.B. 70 kg) ein, erhält man CL =
"totale Körper-Clearance" in den Einheiten ml Blut-Kompartment / min.
Es ist sicherer, Chloroquin oral zu verabreichen, weil die Absorptions-
und Verteilungsraten näher beieinanderliegen ;
-
Maximalkonzentrationen werden in etwa 3 - 5 Stunden nach oraler Einnahme
erreicht.
Die Halbwertszeit von Chloroquin steigt
-
von einigen wenigen Tagen
-
auf Wochen an,
während Plasma-Konzentrationen abnehmen, was den Übergang von
langsamer Verteilung nach noch langsamerer Elimination aus extensiven Gewebereservoirs..
-
Die Halbwertszeiten der abschließenden Elimination liegen zwischen
30 und 60 Tagen,
-
Spuren des Medikaments können im Urin noch über Jahre nach der
therapeutischen Anwendung gefunden werden.
Anreicherung in Gewebe, Gehirn,
Wirbelsäule
(nach Product
Information for chloroquine phosphate (ARALENE) distributed by Sanofi
Winthrop Pharmaceuticals, Park Ave, New York, NY 10016, USA)
Bei Tieren kann man das 200- ... 700-fache der Plasmakonzentration finden
in
Chloroquin wird auch in Leukozyten angereichert.
Die Konzentration in
ist nur das 10- ...30-fache der Konzentration im Plasma.
Erklärung der Begriffe "Clearance", "Verteilungsvolumen" und Eliminationshalbwertszeit
(J. Gruber)
Nach Goodman & Gilman's, Allgemeine Grundlagen, Kapitel "Clinical
Pharmacokinetics" in Leslie Benet Abschnitt "Pharmacokinetics" .
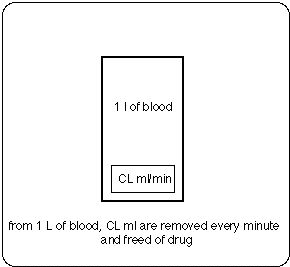
CL = Clearance from blood compartment (ml per minute)
(the notion used is that every minute a volume CL (ml) is removed
(and freed of drug) from the volume of distribution Vss)
Example.
In GG-Appendix II, the "plasma clearance" for cephalexin
is reported as CL/F = 4.3 ml min-1 kg-1,
with 91% of the drug excreted unchanged in the
urine.
For a 70-kg man, the "total body clearance from plasma" CL
= 300 ml/min,
with renal clearance accounting for 91% of this
elimination.
In other words, the kidney is able to excrete cephalexin
at a rate such that approximately 273 ml of plasma would be freed of drug
per minute.
Because clearance usually is assumed to remain constant
in a stable patient, the total rate of elimination of cephalexin will depend
on the concentration of drug in the plasma (equation
1-2).
useful definitions:
-
Clearance
CL = (rate of elimination by specified route) / (Concentration in specified
compartment)
-
Elimination half life
t1/2 = ln2/k = ln2 Vss/CL
Thus
CL = k Vss and
k = CL/Vss (= fraction of Vss removed per minute)
-
Diff. eq. describing elimination:
dm/dt = - k m
(in GG k m is called "rate of elimination")
(equation 1-2)
rate of elimination = C CL =
= C k Vss =
= k C Vss = k m
with the following nomenclature:
C = concentration of drug in blood (g drug/ml blood)
CL = clearance ((ml blood / l volume of distribution) / minute)
k = elimination constant,
m = mass of drug (g)
rate of elimination = dm/dt = change of mass of drug in Vss per unit
time
Abschätzung der Dosis zum Erreichen einer Konzentration von freiem
Chloroquin von 32 microg/ml in Blut, Anreicherung
im Gewebe (200-fach), Gehirm (10-fach)
Während etwa 2 Halbwertszeiten füllt die eingenommene Menge das
Verteilungsvolumen Vss = 100 l/kg 70 kg = 7 103 L.
Wenn
-
100 % des Medikaments bioverfügbar wäre und
-
100 % als freies Chloroquin vorläge (also nicht an andere Moleküle
gebunden),
muß die totale eingenommene Medikamenten-Menge intake1 sein
intake1 = 32 microg/ml Vss = 224 g Basiswirkstoff
Weil aber
-
die Bioverfügbarkeit etwa 100 % ist, aber
-
grob die Hälfte an Plasma-Proteine gebunden ist,
muß die Einnahme gro das Doppelte von intake1 sein:
notwendige Einnahme = 2 intake1 = 448 g.
Damit ergibt die Dosisabschätzung 448 g pro 2 t1/2.
Obwohl das große Verteilungsvolumen andeutet, daß Chloroquin
auch in andere Kompartments als 1. - 4 begibt und
daß die Konzentration in diesen Kompartments wahrscheinlich höher
iat als die Konzentration im Blut, sagen uns die pharmacokinetischen
Daten nicht, wie niedrig die Konzentration im Blut sein kann, damit
eine Konzentration von 32 microg/ml in Bb Zysten infiziertem
Gewebe erreicht wird.
Mit den Anreicherungsdaten von Sanofi und
unter der Annahme einer Eliminationshalbwertszeit t1/2 = 41 + 14 (41 - 14) Tage,
erhält man folgenden Schätzwert für die einzunehmende Dosis
-
Dosis = 4000 (8000) mg/Tag für 32 Microgramm/ml in Blut,
-
Dosis = 20 (40) mg/Tag für 32 Microgramm/ml in Gewebe,
-
Dosis = 400 (800) mg/Tag für 32 Microgramm/ml im Gehirn.
Die Dosis zum Erreichen von 32 Microgramm/ml in Blut liegt
über der Dosis (approximately 1000 mg/Tag),
die für Erwachsene mit Malaria empfohlen wird (siehe auch Medline
Literaturesuche, Stichworte "hydroxychloroquine/adverse effects"[All Fields] AND dosage).
Bei Einnahme von weniger als 4000 (8000) mg pro Tag könnte das Blutkompartment für mobile Spirocheten nicht bakterizid sein, wenn die
Brorsons' in vitro Daten auf in vivo-Fälle anwendbar sind. Man hat aber zu beachten, daß dies eine sehr grobe Abschätzung ist, die darauf abzielt, herauszufinden, ob HCQ als mögliches Mittel gegen Borreliose diskutiert werden kann.
Goodman & Gilman's "Pharmacological Basis of Therapeutics"
Toxizität and Nebenwirkungen
Hohe tägliche Dosen (>250 mg) von Chloroquin oder Hydroxychloroquin
können zu irreversiblen Hör- und Retinaschäden (Retinopathie)
führen.
Bei Dosen von 200 - 400 mg pro Tag) erscheint das Risiko von Ablagerungen in der Hornhaut (corneale Depositionen) und Schädigung des Auges geringer für Hydroxychloroquin als für Chloroquin zu sein.
Retinopathie hängt vermutlich mit der Medikamenten-Anreicherung
in Melanin-reichen Geweben zusammen (Bernstein et al., 1963) und kann vermieden
werden, wenn die täh=gliche Dosis 250 mg oder weniger beträgt
(Medline-Suche nach Dubois,
1978 und nach Rennie, 1993).
Bernstein, H.N., Svaifler, N.J., Rubin, M., and Mausour, A.M.
The ocular deposition of chloroquine. Invest. Ophthalmol. Visual Sci.,
1963, 2:384-392.
Hydroxychloroquin und Lyme
Int Microbiol 2002 Mar;5(1):25-31
Brorson O, Brorson SH.
Department of Microbiology, Vestfold Sentralsykehus, Tonsberg, Norway.
In this work the susceptibility of mobile and cystic forms of Borrelia
burgdorferi to hydroxychloroquine (HCQ) was studied.
-
The minimal bactericidal concentration (MBC) of HCQ against the mobile
spirochetes was
-
> 32 microg/ml at 37 degrees C, and
-
> 128 microg/ml at 30 degrees C.
-
Incubation with HCQ significantly reduced the conversion of mobile spirochetes
to cystic forms. When incubated at 37 degrees C, the MBC was
-
> 8 microg/ml for young biologically active cysts (1-day old), but
it was
-
> 32 microg/ml for old cysts (1-week old).
(compare with effective concentrations
and toxic concentration given in GG)
-
Acridine orange staining, dark-field microscopy and transmission electron
microscopy revealed that the contents of the cysts were partly degraded
when the concentration of HCQ was > or = MBC.
-
At high concentrations of HCQ (256 microg/ml) about 95% of the cysts were
ruptured (250 microg/ml is the toxic concentration).
-
When the concentration of HCQ was > or = MBC, core structures did not develop
inside the cysts, and the amount of RNA in these cysts decreased significantly.
-
Spirochetal structures inside the cysts dissolved in the presence of high
concentrations of HCQ.
-
When the concentration of HCQ was > or = MBC, the core structures inside
the cysts were eliminated.
These observations may be valuable in the treatment of resistant infections
caused by B. burgdorferi, and suggest that a combination of HCQ and a macrolide
antibiotic could eradicate both cystic and mobile forms of B. burgdorferi.
PMID: 12102233 [PubMed - in process]
Weiterführende Literatur
Version: 19. August 2008
Joachim Gruber
Adresse dieser Seite
Home